Precision Urological Oncology and Robotic Surgery
Dr. Tushar Aditya Narain is trained at AIIMS, PGI, UCLH London & Cleveland Clinic USA. 15+ Years Experience. 500+ Successful Robotic Surgeries.

Perspectives from Real Families
Perspectives from Real Families
Hear directly from patients and families about their treatment journey. Every patient's experience is different; these accounts reflect individual cases and do not represent a guarantee of any specific outcome.
Hear directly from patients and families about their treatment journey. Every patient's experience is different; these accounts reflect individual cases and do not represent a guarantee of any specific outcome.

Prostate Cancer Recovery
Chicago to Delhi? Why Mr. Shukla Chose Robotic Surgery In India
✈️International Patient

Kidney Preservation
Satyaki's VHL Journey - Preserving Kidney Function Through Robotic Surgery
🧬Complex Case

Prostate Cancer Recovery
Second Opinions to Surgery: How Mr. Parmar Navigated His Prostate Cancer Decision
🔍Multi-Opinion Journey

Prostate Cancer Recovery
Mr. Singh's Prostate Cancer Journey at Max Hospital
🏥Short Hospital Stay

Prostate Cancer Recovery
Nigeria to Delhi? Why Mr. Uche Chose Robotic Surgery In India
✈️International Patient

Enlarged Prostate (BPH)
10 Years of Prostate Trouble: How Mr. Prasad Found Relief Through Robotic Surgery
⏱️Decade-Long Condition
Prostate Cancer Recovery
Second Opinions to Surgery: How Mr. Parmar Navigated His Prostate Cancer Decision
🔍Multi-Opinion Journey
Kidney Preservation
Satyaki's VHL Journey - Preserving Kidney Function Through Robotic Surgery
🧬Complex Case
Prostate Cancer Recovery
Chicago to Delhi? Why Mr. Shukla Chose Robotic Surgery In India
✈️International Patient
Prostate Cancer Recovery
Second Opinions to Surgery: How Mr. Parmar Navigated His Prostate Cancer Decision
🔍Multi-Opinion Journey
Kidney Preservation
Satyaki's VHL Journey - Preserving Kidney Function Through Robotic Surgery
🧬Complex Case
Prostate Cancer Recovery
Chicago to Delhi? Why Mr. Shukla Chose Robotic Surgery In India
✈️International Patient
These videos are published on Max Healthcare's official YouTube channel. Each patient's experience is unique - outcomes depend on individual health, disease characteristics, and clinical factors. These accounts are not a guarantee of results.
What our patients say on Google
Sharan Bhatia
Prostate Cancer

30 August 2025

I had negligible pain post procedure and surgery was performed in a highly skilled manner with great expertise by Dr Tushar...
Read full review
Hanna Tilabun
Prostate Cancer
15 June 2025
Thushar is not only an exceptionally skilled uro-oncologist and robotic surgeon but also a remarkably humble and compassionate physician...
Read full review
MD NABEEL AKHTAR
Prostate Cancer
08 March 2025
Exceptional Robotic Surgery by Dr. Tushar Aditya Narain
Dr. Tushar Aditya Narain performed a highly complex robotic surgery...
Read full review
What our patients say on Google
Sharan Bhatia
Prostate Cancer
30 August 2025
I had negligible pain post procedure and surgery was performed in a highly skilled manner with great expertise by Dr Tushar...
Read full review
Hanna Tilabun
Prostate Cancer
15 June 2025
Thushar is not only an exceptionally skilled uro-oncologist and robotic surgeon but also a remarkably humble and compassionate physician...
Read full review
MD NABEEL AKHTAR
Prostate Cancer
08 March 2025
Exceptional Robotic Surgery by Dr. Tushar Aditya Narain
Dr. Tushar Aditya Narain performed a highly complex robotic surgery...
Read full review
What our patients say on Google
Sharan Bhatia
Prostate Cancer
30 August 2025
I had negligible pain post procedure and surgery was performed in a highly skilled manner with great expertise by Dr Tushar...
Read full review
Hanna Tilabun
Prostate Cancer
15 June 2025
Thushar is not only an exceptionally skilled uro-oncologist and robotic surgeon but also a remarkably humble and compassionate physician...
Read full review
MD NABEEL AKHTAR
Prostate Cancer
08 March 2025
Exceptional Robotic Surgery by Dr. Tushar Aditya Narain
He performed a highly complex robotic surgery...
Read full review
Understand Your Journey

Know More About Dr. Tushar - The Surgeon Who Trains Surgeons
Official Robotic Trainer for Intuitive Surgical.

See How Precision Robotics Leads To Faster Recovery
Get back to your family in days, not weeks.

Curated Guides by Dr. Tushar
Explore articles, videos and quiz!
Explore Curated Guides by Dr. Tushar
Explore articles, videos and quiz!
Precision Oncology: Specialized Robotic Solutions
Precision Oncology: Specialized Robotic Solutions
We don't just treat the disease; we preserve the individual. By combining world-class robotic precision with a commitment to functional recovery, Dr. Tushar & Care Team provide personalized roadmaps to a cancer-free life.
We don't just treat the disease; we preserve the individual. By combining world-class robotic precision with a commitment to functional recovery, Dr. Tushar & Care Team provide personalized roadmaps to a cancer-free life.






Online Consultations Available
Book a video consultation anytime, from anywhere
Book a video consultation anytime, from anywhere
Tremor-Free Precision
Filter out human tremor and use 3D HD vision to target cancer with microscopic accuracy.
Recovery in Days
Typically home in 1-2 days. Tiny keyhole incisions mean minimal pain and reduced blood loss.
Preserving What Matters
Meticulous nerve-sparing technique designed to preserve your urinary control and sexual function.
Trained to Teach
The surgeon trusted to train others. Dr. Tushar is an official Proctor and UK-fellowship trained.
Tremor-Free Precision
Filter out human tremor and use 3D HD vision to target cancer with microscopic accuracy.
Recovery in Days
Typically home in 1-2 days. Tiny keyhole incisions mean minimal pain and reduced blood loss.
Preserving What Matters
Meticulous nerve-sparing technique designed to preserve your urinary control and sexual function.
Trained to Teach
The surgeon trusted to train others. Dr. Tushar is an official Proctor and UK-fellowship trained.
Video Series - Decoding Robotic Surgery
Myth vs. Reality: Who Is In Charge?
Does the robot think? Absolutely not. See how Dr. Tushar uses the Da Vinci system as a precision tool, maintaining 100% control of every movement.
Series 1 - Part 1 of 3
Myth Busted: Who Operates?
Think the robot does the surgery? Think again. Dr. Tushar explains why the machine is zero percent autonomous and the surgeon is the only pilot.
Duration of video is 34 seconds
Series 1 - Part 1 of 3
Myth Busted: Who Operates?
Think the robot does the surgery? Think again. Dr. Tushar explains why the machine is zero percent autonomous and the surgeon is the only pilot.
Duration of video is 34 seconds
Series 1 - Part 2 of 3
The Cockpit: Total Control
Step into the pilot’s seat. See the console where Dr. Tushar’s hand movements are translated instantly into microscopic, tremor-free precision.
Duration of video is 23 seconds
Series 1 - Part 2 of 3
The Cockpit: Total Control
Step into the pilot’s seat. See the console where Dr. Tushar’s hand movements are translated instantly into microscopic, tremor-free precision.
Duration of video is 23 seconds
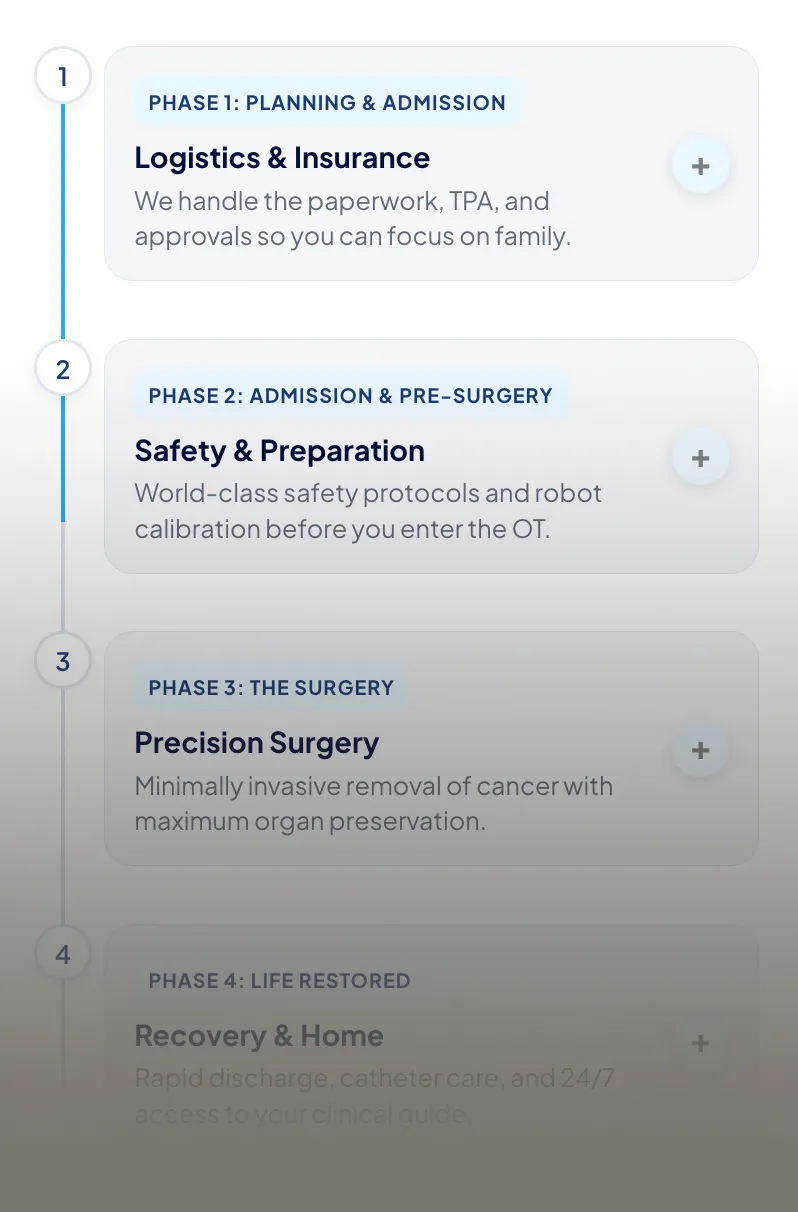
You Don't Just Get a Surgeon. You Get a System.
Dr. Tushar leads the surgery, but our team manages the journey. From handling paperwork to daily recovery advice, we manage the logistics so you can focus on healing.


You Don't Just Get a Surgeon. You Get a System.
Dr. Tushar leads the surgery, but our team manages the journey. From handling paperwork to daily recovery advice, we manage the logistics so you can focus on healing.
You Don't Just Get a Surgeon. You Get a System.
Dr. Tushar leads the surgery, but our team manages the journey. From handling paperwork to daily recovery advice, we manage the logistics so you can focus on healing.


